This 15-year-old male was referred in 1975 with the Prune Belly Syndrome. At age 2 weeks, bilateral nephrostomies had been performed and thereafter an ileal loop which was unfortunately placed in backwards and did not drain well. A second ileal loop was later performed but it drained poorly also.
The long defunctioned bladder would hold only 100 ml at age 15, even filling with a water pressure 4 feet above his bladder level. Cystoscopy disclosed a type 3 urethral valve which was opened endoscopically in 4 quadrants.
The bowel segment was usuable after reversing its orientation to flow left to right! There was ureteropelvic junction obstruction on both sides. The left colic artery was placed behind the new renal pelvic junction. Both renal pelves were trimmed. The loop was tapered. A psoas hitch was performed to stabilize the new “ureter” reimplant.
Operative time was 11 hours. Blood replacement was with washed red cells to minimize sensitization in view of future renal transplantation.
At 1.5 years after his undiversion surgery, his chemistries were: BUN 40, creatinine 2.0, CO2 19, creatinine clearance 61 liters.
Anatomy (Select Image for High-quality Version). (Top) Preoperative anatomy. (Bottom) Postoperative anatomy.
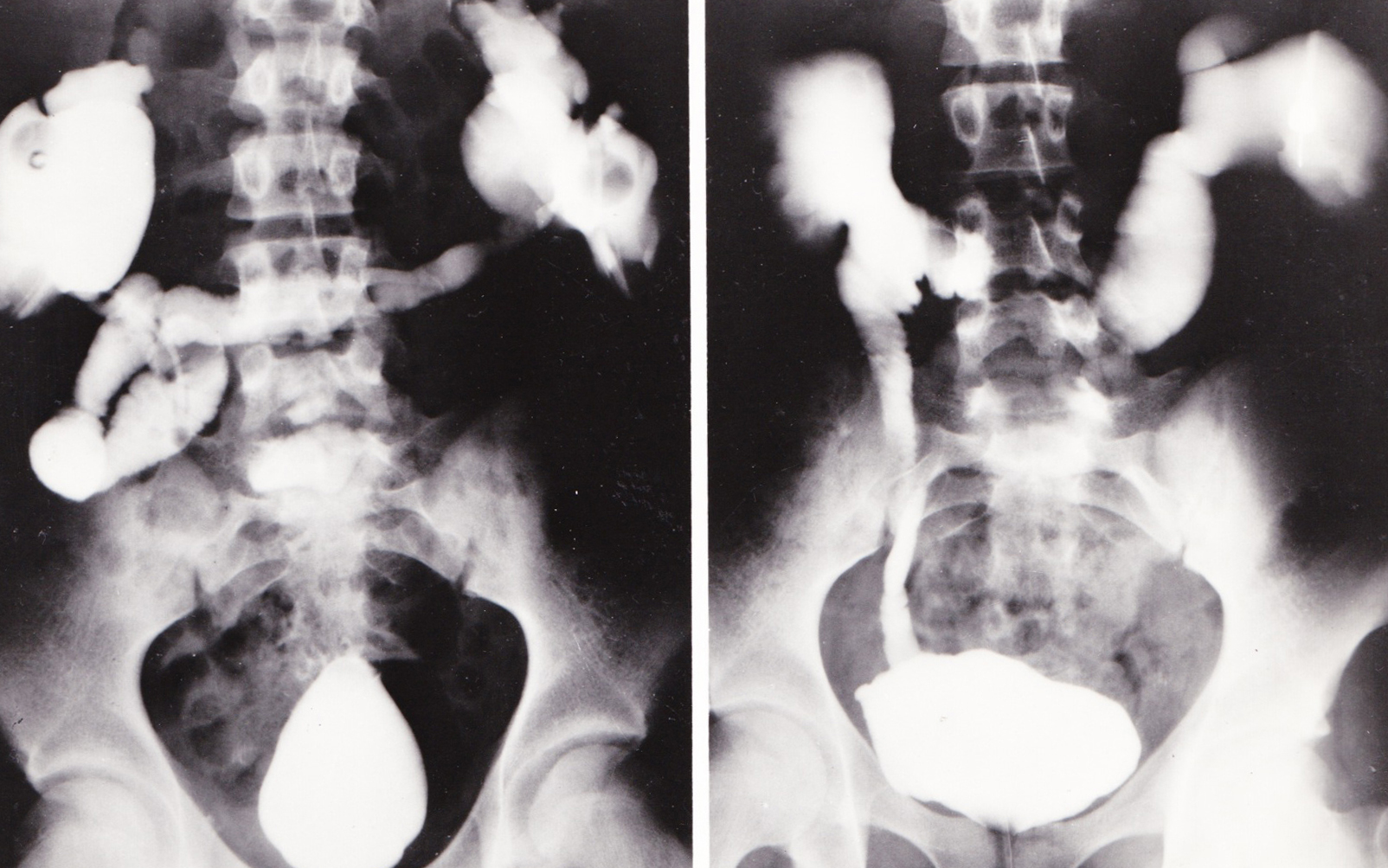
X-rays (Select Image for High-quality Version). (Left) Antegrade nephrostogram via needle in left kidney. Note small,smooth walled capacity bladder not in use since infancy. (Right) Anategrade study via left kidney 2 years after undiversion at age 15 years. Note now normal bladder size.
Four years later he returned in renal failure (creatinine 12). A living related donor renal transplant from an older brother was done at age 25 years. It was an excellent match; his serum creatinine was 1.2 a year later; he did experience aseptic necrosis of his femoral heads.